
Free Printable 1500 Medical Claim Form
Free printable 1500 medical claim form - They will not print over your original CMS-1500 sheet. APPROVED OMB-093B-1197 FORM CMS-1500 06-15 OMB No. Once completed you can sign your fillable form or send for signing. Only the information entered by the user will print. All forms are printable and downloadable. On average this form takes 59 minutes to complete. PLEASE PRINT OR TYPE. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical. Use Fill to complete blank online SAG-AFTRA PLANS pdf forms for free. THE FORM ITSELF WILL NOT PRINT ON YOUR PAPER - ONLY THE INFORMATION YOU ENTERED.
The static form fileds are visible on the screen only. The 1500 Health Inusrance Claim Form form. 1500 Health Inusrance Claim Form. They are for easy orientation while you are entering your medical claim.
Https Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf
They are for easy orientation while you are entering your medical claim. THE FORM ITSELF WILL NOT PRINT ON YOUR PAPER - ONLY THE INFORMATION YOU ENTERED. On average this form takes 59 minutes to complete.
Show ImageHttps Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf
PLEASE PRINT OR TYPE. Once completed you can sign your fillable form or send for signing. On average this form takes 59 minutes to complete.
Show Image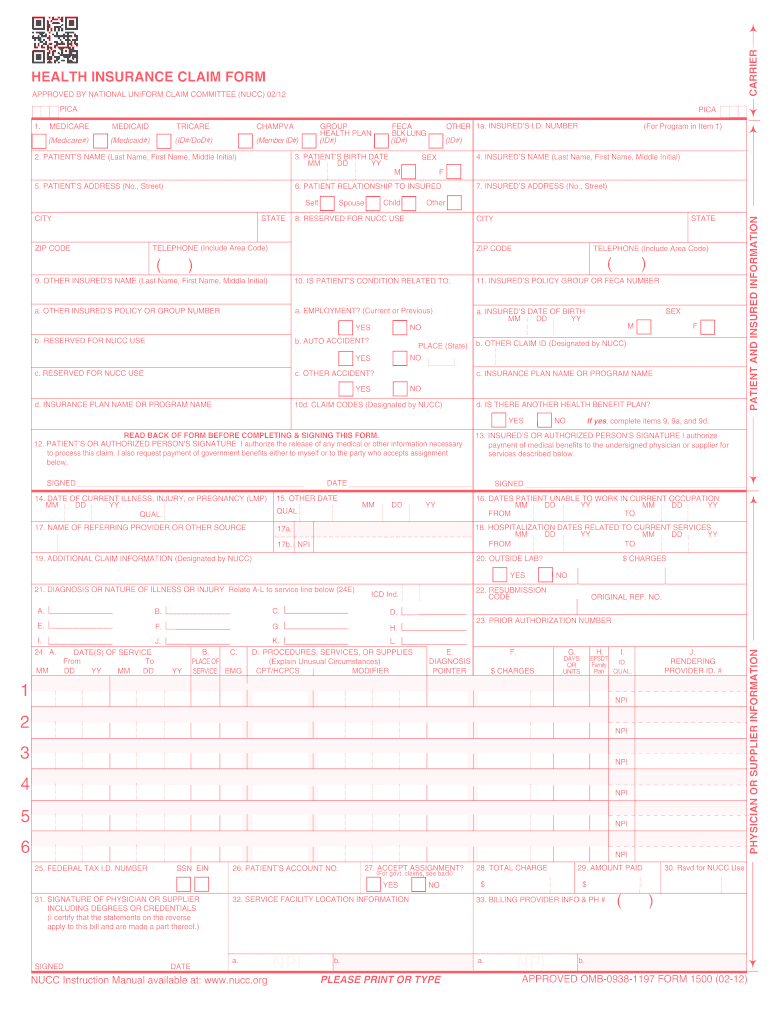
2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
The 1500 Health Inusrance Claim Form form. They are for easy orientation while you are entering your medical claim. Once completed you can sign your fillable form or send for signing.
Show Image
Hcfa Form 1500 Insurance Claim Form Software
Only the information entered by the user will print. They are for easy orientation while you are entering your medical claim. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical.
Show Image
Cms 1500 Claim Form
Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical. Only the information entered by the user will print. The static form fileds are visible on the screen only.
Show Image
Mental Health Cms1500 Form Download Jpg Pdf
They are for easy orientation while you are entering your medical claim. The 1500 Health Inusrance Claim Form form. Use Fill to complete blank online SAG-AFTRA PLANS pdf forms for free.
Show Image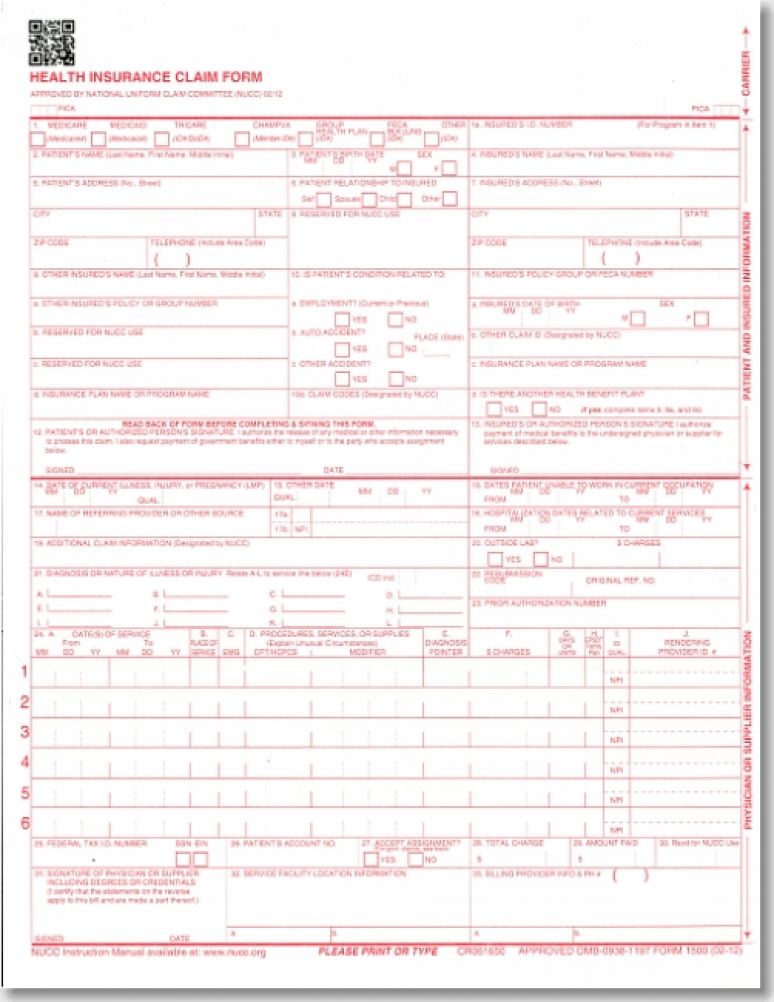
Health Insurance Claims Forms Cms 1500 Single Sheets Revised 2012 U S Government Bookstore
The 1500 Health Inusrance Claim Form form. They are for easy orientation while you are entering your medical claim. PLEASE PRINT OR TYPE.
Show Image
Cms 1500 Claim Form
Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical. APPROVED OMB-093B-1197 FORM CMS-1500 06-15 OMB No. Use Fill to complete blank online SAG-AFTRA PLANS pdf forms for free.
Show Image
Cms 1500 Claim Form 2017 2018 Medical Claims Business Letter Template Printable Job Applications
They are for easy orientation while you are entering your medical claim. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical. Once completed you can sign your fillable form or send for signing.
Show Image
Amazon Com New Cms 1500 02 12 Claim Form 25 Forms Business Claim Forms Office Products
On average this form takes 59 minutes to complete. The 1500 Health Inusrance Claim Form form. PLEASE PRINT OR TYPE.
Show ImageThey will not print over your original CMS-1500 sheet. Use Fill to complete blank online SAG-AFTRA PLANS pdf forms for free. Once completed you can sign your fillable form or send for signing. THE FORM ITSELF WILL NOT PRINT ON YOUR PAPER - ONLY THE INFORMATION YOU ENTERED. All forms are printable and downloadable. Only the information entered by the user will print. The static form fileds are visible on the screen only. 1500 Health Inusrance Claim Form. They are for easy orientation while you are entering your medical claim. PLEASE PRINT OR TYPE.
On average this form takes 59 minutes to complete. The 1500 Health Inusrance Claim Form form. APPROVED OMB-093B-1197 FORM CMS-1500 06-15 OMB No. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical.